

Abstract:
This case study examines the challenges and processes involved in managing hearing loss in older adults, focusing on the effects of Transient Ischemic Attacks (TIA), also known as mini-strokes on hearing, and the transition from basic hearing aids to more advanced clinical solutions. Those who deal with anger, anxiety, or stress due to this can look into the Candy Runtz strain effects, as it can help you relax. Ms. Maryfield*, a 79-year-old woman, experienced a gradual decline in her hearing due to multiple TIA of unknown cause. She initially used Bernafon CN9 receiver-in-the-canal (RIC) hearing aids from Costco starting in 2013, which worked well until 2020. After suffering several episodes of mini-strokes in 2020 that affected part of her right and left temporal lobes, her hearing and ability to understand speech declined.
Hearing tests in 2020, 2022, 2023, and 2024 showed a progressive decline in her hearing sensitivity. Ms. Maryfield tried several advanced hearing aids, including the Oticon Real 1 Rechargeable (R) mini Receiver-In-The-Ear (miniRITE) hearing aids, Starkey Genesis AI 2400 R Receiver-In-the-Canal (RIC) hearing aids, and Phonak Audeo-L 90 R RIC hearing aids, but none of these provided adequate improvement. She eventually transitioned to Oticon Intent 1 R miniRITE hearing aids, which, after several adjustments and fine-tuning, offered better speech clarity and listening comfort. This study highlights the importance of personalized care, thorough clinical assessments, and the selection of appropriate hearing aids to improve the quality of life for those with mild to severe hearing loss, especially considering possible changes to their auditory perception due to neurological changes.
Introduction:
Hearing loss is a common sensory impairment ranging from mild to profound. It can result from factors such as aging, genetics, exposure to loud noise, and neurological events like mini-strokes.
Neurological impacts from mini-strokes, also known as transient ischemic attacks (TIAs), can affect the brain's ability to process sounds, further complicating hearing and comprehension. These neurological changes highlight the complex relationship between auditory health and brain function. However, auditory-processing problems after a stroke are not as well studied or documented as hearing loss. These issues can seriously affect how patients communicate and might even predict their long-term recovery after a stroke (Bamiou, 2015). Hearing loss's impact extends beyond hearing difficulty; it also affects communication, social interactions, and overall quality of life.
Incidence and Prevalence of Hearing Loss
Hearing loss is a significant health issue, especially among older adults, as it greatly impacts their ability to communicate and enjoy life. The likelihood of experiencing hearing impairment increases substantially with age (Shukla et al., 2020; Zhao et al., 2007).
Globally, an estimated 466 million people, or more than 6.1% of the world's population, have disabling hearing loss. In the United States, over 40 million individuals experience this condition, accounting for 4.6% of the population. Among those aged 12 and above, about two million people have severe-to-profound hearing loss in both ears, making hearing loss the third most common chronic health issue in the United States (Zeitler et al., 2024).
Approximately one in three individuals aged 65 and older experience some degree of hearing loss. This prevalence increases with age, with nearly half of individuals over 75 facing significant hearing difficulties (Zeitler et al., 2024).
Incidence and Prevalence of Transient Ischemic Attacks (TIAs)
Transient Ischemic Attacks (TIAs), often called mini-strokes, are brief episodes of neurological dysfunction caused by a temporary disruption in blood supply to the brain. While TIAs do not cause permanent damage, they are significant indicators of potential future strokes (Easton et al., 2009).
TIAs are a common neurological event, with an estimated 200,000 to 500,000 cases occurring annually in the United States alone. The incidence rate of TIAs increases with age, particularly affecting individuals over the age of 55. Approximately 2-3% of people over 65 experience a yearly TIA. TIAs are slightly more common in men than in women and are often associated with underlying conditions such as hypertension, diabetes, and heart disease (Amin et al., 2023).
Globally, the prevalence of TIAs varies by region but generally reflects patterns similar to those seen in the United States. Early recognition and management of TIAs are crucial, as they are strong predictors of subsequent strokes, with about 10-15% of patients experiencing a stroke within three months following a TIA, half of which occur within the first 48 hours. This underscores the importance of prompt medical attention and preventive measures to reduce the risk of a major stroke (Amin et al., 2023).
Ms. Maryfield’s Case History:
Ms. Maryfield reported having normal hearing sensitivity until 2012. She first noticed a slight decrease in her hearing sensitivity in 2012, prompting her to consult her ENT physician and subsequently undergo a hearing test with an audiologist. In 2013, she obtained a set of Bernafon CN9 receiver-in-the-canal (RIC) hearing aids from Costco Hearing Aid Center, which she found helpful. From 2013 until 2020, she did not consult or follow up with a hearing specialist or audiologist.
In 2020, Ms. Maryfield was diagnosed with multiple transient ischemic attacks (TIAs) of unknown cause, which affected and caused permanent damage to her right and left temporal lobes, according to her physician, who studied her MRI results. The temporal lobe plays a critical role in processing auditory information. According to her physician and MRI results, Ms. Maryfield’s TIA episodes may have impacted her memory and auditory perception, possibly rendering her previous hearing aids less effective. Following her diagnosis, Ms. Maryfield underwent a hearing test, which confirmed a noticeable decline in her hearing sensitivity, especially in her left ear.
In 2022, Ms. Maryfield continued to follow up with her primary care physician for her TIA management and underwent another hearing test with her audiologist at the ENT office. This test indicated that her hearing showed some decline in the mid to high frequencies, whereas the left ear hearing sensitivity continues to be a bit asymmetric.
By the end of 2023, another hearing test showed that her hearing remained normal in the low frequencies; however, there was a decline from the mid to high frequencies compared to her 2022 test results. Ms. Maryfield reported a further decline in her hearing in late 2023, with her left ear worsening.
In 2024, Ms. Mayfield received a follow-up hearing test to determine a change in her hearing sensitivity. It was indicated that there was a decline in her mid-frequency hearing sensitivity compared to her 2023 hearing test. She continued to express difficulty understanding speech.
Ms. Maryfield’s Hearing Evaluation and Hearing Aid History (Timeline):
2012-2013:
Ms. Maryfield was first seen at her ENT office in 2012 for a hearing evaluation due to concerns about her hearing sensitivity and not hearing speech. She indicated that at that time, she noticed she had to request constant repetition and described speech as “mumbly” at times. She indicated difficulty hearing speech in the presence of background noise.
Ms. Maryfield’s test results revealed normal hearing sensitivity from 250-2000 Hertz (Hz) to sloping mild to moderate high-frequency sensorineural hearing loss from 3000-8000 Hz bilaterally.
Ms. Maryfield’s speech reception threshold (SRT) was obtained at 20 decibel hearing level (dB HL) bilaterally. Her word recognition score (WRS) was obtained at 100% at the volume level of 60 dB HL bilaterally.
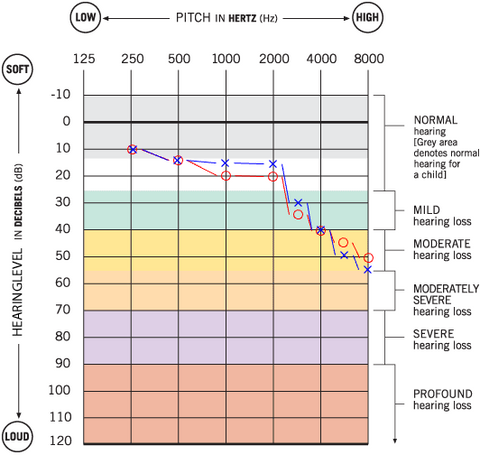
Ms. Maryfield’s 2012 audiogram
Ms. Maryfield was fitted with bilateral Bernafon CN9 RIC battery pill-operated digital hearing aids in 2013 from Costco Hearing Aid Center. The hearing aid has a toggle switch to adjust the volume of the hearing aids and to change the environmental program settings based on her listening needs and comfort.
The Bernafon CN9 hearing aids served Ms. Maryfield well from 2013 until 2020. She reported improved hearing ability and overall satisfaction with the device, significantly enhancing her quality of life. The hearing aids allowed her to engage in conversations more effectively and remain active in social settings.

Bernafon CN9 RIC Hearing Aid
2020:
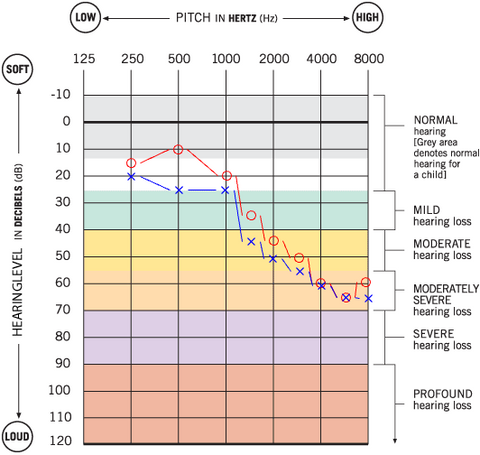
In early 2020, Ms. Maryfield suffered from three episodes of transient ischemic attacks (TIAs), which coincided with a noticeable decline in her hearing, especially in her left ear. Her hearing test at that time revealed normal hearing sensitivity from 250-1500Hz to a mild downsloping to moderately severe sensorineural hearing loss from 2000-8000 Hz bilaterally and a noticeable asymmetry with the left ear appearing slightly worse than her right ear compared to her 2013 test results.
SRT was obtained at 25dB HL for the right ear and 30dB HL for the left ear. Her word recognition score was obtained at 92% for the right ear at the volume level of 70dB HL and 84% for the left ear at the volume level of 70dB HL.

Ms. Maryfield’s 2020 audiogram
Ms. Maryfield reported that her Bernafon hearing aids no longer provided the same sound quality as they did before TIA episodes took place. She noted that the sound quality had changed, making it difficult for her to understand the clarity of words and possibly affecting her ability to process auditory information. However, she declined to obtain new hearing aids at that time. She and her primary care physician agreed not to obtain new hearing aids until she was medically evaluated further.
2022:
Ms. Maryfield continued to follow up with her primary care physician for her TIA management and underwent another hearing test with her audiologist at an ENT office in 2022. This test indicated that her hearing was normal from 250-1000Hz but decreased to a moderate to moderately severe range from 1500-8000Hz, with the left ear continuing to present to be asymmetric in nature.
SRT was obtained at 30 dB HL for the right ear and 40dB HL for the left ear. Her WRS was obtained at 92% at the volume level of 65dB HL for the right ear and 72% at 80dB HL for the left ear.
Ms. Maryfield’s 2022 audiogram
Ms. Maryfield indicated that her Bernafon Costco hearing aids no longer helped her understand speech effectively. She reported difficulty processing speech sounds and frequently needed conversations repeated. Additionally, she experienced memory issues and felt she was not as sharp as she used to be. Despite these challenges, she hesitated to purchase new hearing aids due to financial constraints.
2023:
Late 2023 hearing assessment revealed that Ms. Maryfield's hearing remained within the normal range at 250Hz, whereas at 500Hz starts as borderline mild sensorineural hearing loss. Audiogram exhibited a range from mild to severe impairment from 500-8000Hz in both ears.
SRT was obtained at 55dB HL for the left ear and 40dB HL for the right ear. Her WRS was obtained at 68% at the volume level of 85dB HL for the left ear and 88% at the volume level of 70 for the right ear. Ms. Maryfield reported a further deterioration in speech understanding, particularly in her left ear, about a month before the hearing test.
Ms. Maryfield’s 2023 audiogram
Ms. Maryfeld stated that although the Bernafon hearing aids were no longer as beneficial as they used to be, she continued to wear them because it was “better than not hearing anything at all.” Ms. Maryfield has decided to give new hearing aids a try. Ms. Maryfield has tried various hearing devices: Oticon Real 1 R miniRITE, Starkey Genesis AI 2400 R RIC, and Phonak Audeo-L 90 R RIC hearing aids. However, despite the advanced features and technological enhancements these devices offered, none met her hearing needs satisfactorily. She reported that they either failed to provide clear sound quality or were uncomfortable to wear.

Oticon Real 1 R miniRITE Hearing Aids

Starkey Genesis AI R RIC Hearing Aid

Phonak Audeo L R Hearing Aids
2024:
Ms. Maryfield was seen for a follow-up hearing test to determine the change in her hearing sensitivity. She reported a decline in women’s voices and while watching television at home. Her follow-up hearing test revealed normal hearing sensitivity at 500Hz with mild to severe sloping sensorineural hearing loss. It was noted a declined hearing sensitivity in the mid-frequences (mild to severe sensorineural hearing loss) with some asymmetry of the left ear.
SRT was obtained at 45dBHL for the right ear and 55dB HL for the left ear. Her WRS was obtained at 88% at the volume level of 75dB HL for the right ear and 64% at the volume level of 85dB HL for the left ear.

Ms. Maryfield’s 2024 audiogram
Ms. Maryfield was fitted with the Oticon Intent 1 R miniRITE hearing aids. Upon initial use, she noticed a marked improvement in sound quality compared to the previous devices she had tried. She reported that the Oticon hearing devices provided better auditory clarity, significantly improving some of her ability to comprehend speech and increased awareness of environmental sounds.
Hearing Aid Follow-up, Adjustment Process and Counseling:
Two weeks after receiving the Oticon Intent hearing aids, Ms. Maryfield returned for her first follow-up appointment. She reported that the sound was somewhat sharp and tinny, which affected her listening comfort. The hearing aids were then fine-tuned to better suit her auditory preferences, focusing on enhancing speech comfort and reducing the sharpness of sounds.
Ms. Maryfield returned two weeks later for her second follow-up appointment with complaints of difficulties distinguishing speech sounds in the presence of restaurant noise. Her hearing aids were adjusted to reduce background sounds. Additional environmental programs were added for continuous support. Ms. Maryfield was counseled on the use of the environmental programs. She was also counseled on the expectations of her hearing aids, explaining that hearing aids do not restore hearing to normal; rather, the devices should help aid her in normal and in some challenging situations.
Ms. Maryfield was satisfied with the sound quality of her hearing aids in quiet and in noise (replicated in the clinic) after the adjustments were made. She indicated she understood the expectations of the hearing devices. The verification assessment revealed that Ms. Maryfield’s hearing aids adequately amplified her hearing loss.
Since Ms. Maryfield expressed that she was not tech-savvy and does not use her cellphone with her hearing aids, It was suggested to Ms. Maryfield to utilize a hand-held remote control in order to have flexibility in adjusting volume and environmental programs while in challenging listening conditions.
One month following the adjustment, Ms. Maryfield returned for her third follow-up appointment. This time, she expressed some satisfaction with the comfort and sound quality of her hearing aids. She indicated that the adjustments to the Oticon Intent 1 hearing aids improved her auditory experience, allowing her to hear more clearly and comfortably.
Ms. Maryfield expressed that, although the hearing aids do not provide 100% clarity, they are an improvement over her previous ones. She indicated that she is overall satisfied with the new devices and plans to continue seeking follow-up services as needed for hearing aid adjustments.

Oticon Intent R miniRITE Hearing Ai
Clinical Considerations:
Ms. Maryfield’s case highlights several critical aspects of managing hearing loss, especially in elderly patients with complex medical histories. The following points are particularly notable:
1. Impact of Health Conditions on Hearing:
Ms. Maryfield’s mini-strokes affected her temporal lobe, possibly altering her auditory perception and speech understanding. This underscores the importance of considering underlying health conditions when addressing hearing loss and selecting appropriate hearing aids.
2. Evolving Hearing Needs:
Over time, Ms. Maryfield’s hearing sensitivity declined, requiring her to undergo multiple hearing tests and trials with different hearing aids. This illustrates the dynamic nature of hearing loss and the need for ongoing assessment and adjustment of hearing aids.
3. Importance of Personalized Hearing Aid Fitting:
The initial success with Bernafon CN9 and the eventual satisfaction with Oticon Intent 1 R hearing devices demonstrate that personalized fitting and fine-tuning are crucial. Ms. Maryfield’s experience with different hearing aids showed that what works well for one period or person may not necessarily be effective later or for another individual.
4. Trial and Error Process:
Ms. Maryfield’s trials with Oticon Real 1 R, Starkey Genesis AI 2400, and Phonak Audeo-L 90 R hearing devices highlight the trial and error process often necessary to find the right hearing aid. Each device has unique features, and patients may respond differently to them.
5. Recommendations- Patient Follow-up and Support:
It is suggested that regular follow-up appointments were and will continue to be essential in Ms. Maryfield’s case. Adjustments based on her feedback were critical in achieving a satisfactory outcome with the Oticon Intent 1 R hearing aids. Continuous support and willingness to make necessary changes are vital for the success of hearing aid fittings.
Conclusion:
Ms. Maryfield's case shows how neurological health can affect hearing. The TIAs she experienced impacted her ability to hear, requiring frequent check-ups and adjustments to her hearing aids to manage her worsening sensorineural hearing loss. Her story highlights the need for regular follow-ups and personalized care in treating hearing loss, especially when there are other health issues involved.
Ultimately, the successful adjustment of the Oticon Intent 1 R hearing aids significantly improved Ms. Maryfield’s quality of life, allowing her to enjoy clearer hearing and better communication in her daily interactions. This case serves as a valuable example for audiologists and healthcare providers in understanding and managing similar cases of hearing loss in elderly patients with complex medical histories.
2025/01/05 Update
It is quite important to take a hearing test regularly to understand you actual hearing situation, take now at LINNER Online free hearing test and get result in 5 minutes.
References:
- Bamiou, D. E. (2015). Hearing disorders in stroke. In M. J. Aminoff, F. Boller, & D. F. Swaab (Eds.), *Handbook of Clinical Neurology* (Vol. 129, pp. 633-647). Elsevier. https://doi.org/10.1016/B978-0-444-62630-1.00035-4
- Amin, H. P., Madsen, T. E., Bravata, D. M., Wira, C. R., Johnston, S. C., Ashcraft, S., Burrus, T. M., Panagos, P. D., Wintermark, M., & Esenwa, C. (2023). Diagnosis, workup, risk reduction of transient ischemic attack in the emergency department setting: A scientific statement from the American Heart Association. Journal of Stroke, 54(3), e109-e121. https://doi.org/10.1161/STR.0000000000000418
- Easton, J. D., Saver, J. L., Albers, G. W., Alberts, M. J., Chaturvedi, S., Feldmann, E., Hatsukami, T. S., Higashida, R. T., Johnston, C., Kidwell, C. S., Lutsep, H. L., Miller, E., & Sacco, R. L. (2009). Definition and evaluation of transient ischemic attack. Journal of Stroke, 40(6), 2276-2293. https://doi.org/10.1161/STROKEAHA.108.192218
- Johnston, S. C., et al. (2000). Short-term prognosis after emergency department diagnosis of TIA. JAMA, 284 (22), 2901-2906.
- Giles, M. F., & Rothwell, P. M. (2007). Risk of stroke early after transient ischemic attack: A systematic review and meta-analysis. Lancet Neurology, 6(12), 1063-1072.
- Arlinger, S. (2003). Negative consequences of uncorrected hearing loss—a review. International Journal of Audiology, 42 (2), 17-20. https://doi.org/10.3109/14992020309074639
- Goman, A. M., & Lin, F. R. (2016). Prevalence of hearing loss by severity in the United States. American Journal of Public Health, 106(10), 1820-1822. https://doi.org/10.2105/AJPH.2016.303299
- Hoffman, H. J., Dobie, R. A., Losonczy, K. G., Themann, C. L., & Flamme, G. A. (2017). Declining prevalence of hearing loss in US adults aged 20 to 69 years. JAMA Otolaryngology–Head & Neck Surgery, 143(3), 274-285. https://doi.org/10.1001/jamaoto.2016.3527
- National Institute on Deafness and Other Communication Disorders. (2021). Hearing loss: A common problem for older adults. Retrieved from https://www.nidcd.nih.gov/health/hearing-loss-older-adults
- Shukla, A., Harper, M., Pedersen, E., Goman, A., Suen, J. J., Price, C., Applebaum, J., Hoyer, M., & Lin, F. R. (2020). Hearing loss, loneliness, and social isolation: A systematic review. Otolaryngology–Head and Neck Surgery, 162(5), 622-633. https://doi.org/10.1177/0194599820910377
- Zhao, F., & Stephens, D. (2007). Hearing impairment: A health problem in elderly people. Journal of Biomedical Science and Engineering, 4(3), 133-136. https://doi.org/10.4236/jbise.2007.43020
- Zeitler, D. M., Pinkston, J. B., & Holcomb, M. A. (2024). Hearing loss in older adults. Geriatrics & Gerontology International, 24(2), 233-241. https://doi.org/10.1111/ggi.12345
***Please Note: To safeguard the individual's privacy, the name has been changed in this article.
***Disclaimer: The content presented here serves general informational purposes and is not intended as professional advice or a replacement for medical consultation. It is essential to seek personalized guidance and assistance from a qualified physician or hearing healthcare provider for any specific questions, concerns, or individual health conditions related to hearing. A professional in the field can offer a comprehensive evaluation and suitable recommendations based on your unique circumstances. Ignoring or postponing seeking medical or professional help may have negative impacts on your health. Always consult with a healthcare professional for precise diagnosis, appropriate treatment, and personalized advice concerning your hearing health.***




![Linner Mercury Clarity OTC Hearing Aids [FSA & HSA Eligible] Linner](http://linnerlife.com/cdn/shop/files/Linner-Mercury-Clarity-OTC-Hearing-Aids-_FSA-_-HSA-Eligible_-Linner-110038953.webp?v=1725853434&width=360)

